Epidemiology
Learning objectives
By the end of this session, trainees need to understand the:
- Global and the national burden of leishmaniasis
- Geographic distribution of the disease
Recommended facilitation technique
- Make participants read the participant manual
- Arrange a team work to study the world and Ethiopia map on the distribution of disease and identify endemic spots, naming the countries and places
Use map on the supplement power point to demonstrate and explain the distribution of the disease
|
Leishmaniasis occurs in 101 countries and territories – tropics and subtropics – globally. While the population at risk is estimated to be over 350 million, 0.2-0.4 million VL and 0.7-1.2 million CL new cases occur every year. Visceral leishmaniasis, also called kala-azar, is observed to occur in about 70 countries and 200million population at risk. Annually 20,000 to 30,000 deaths occur. Ninety percent of the case load is reported from six countries – India, Bangladesh, Sudan, South Sudan, Ethiopia and Brazil (see Map 1). The term Kala-azar is from Hindu for “black fever” as the disease causes darkening of the skin which is historically related to the massive outbreaks in the region in the past. |
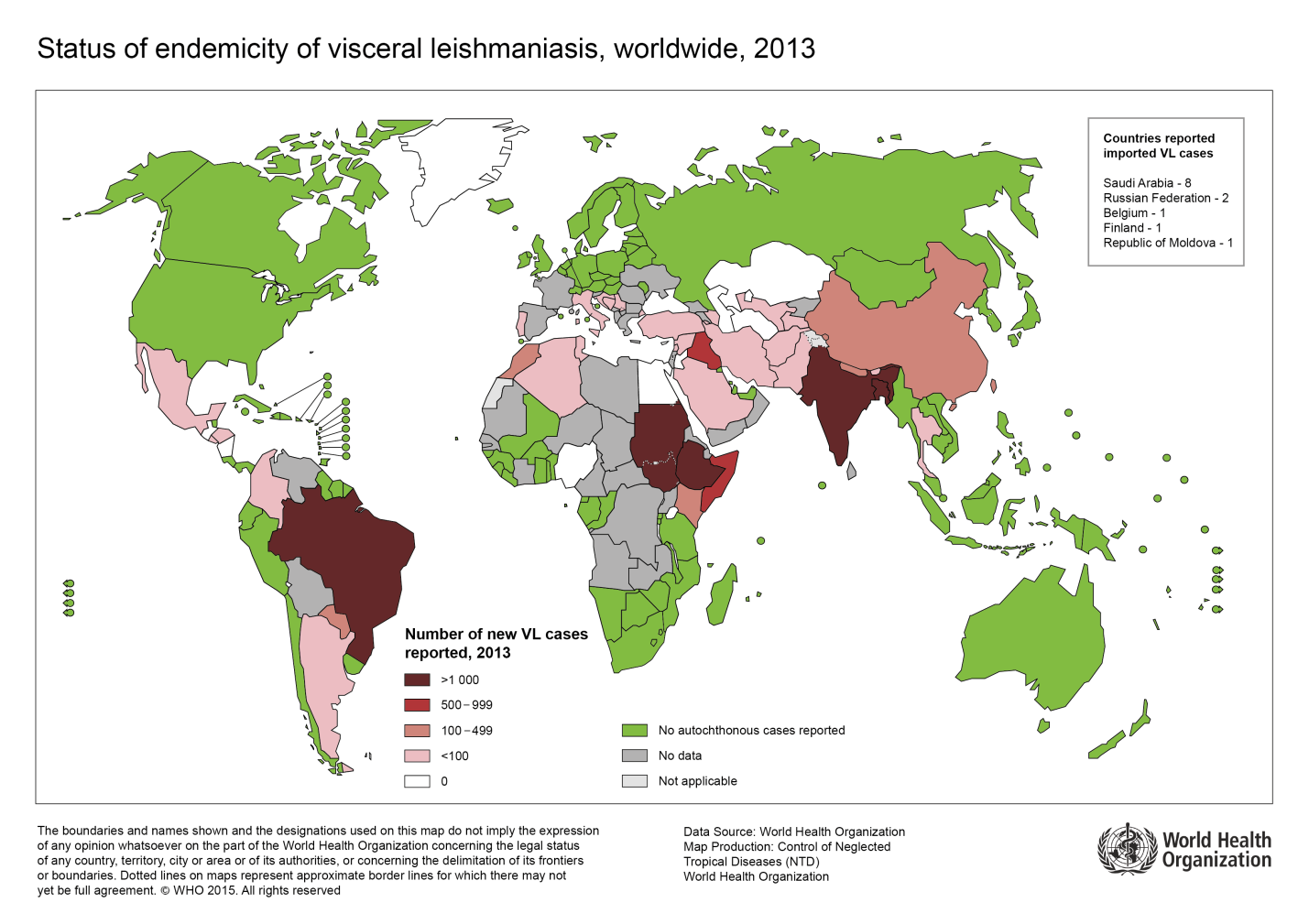 |
| Map 1: Geographic distribution of visceral leishmaniasis. (Reprinted from Desjeux P. Leishmaniasis. Nat Rev Microbiol 2004;2:692; with permission.) |
Epidemiology in Ethiopia
|
VL is found in five administrative regions in Ethiopia – Amhara, Tigray, Southern nations, nationalities and people’s, Oromia and Somalia regions (see Map 2). Exact burden of the diseases is not known due to the under reporting and poor surveillance system. But the estimated annual incidence is 2000-4500 cases. The main endemic spot is the Northwest low land areas bordering Sudan. Young adult (age range from 20-30years) male populations are mainly affected in this region. Population migration related to daily labor work in cash crop farm land areas in this region is the main risk factor for infection. Estimates of 300,000 to 500,000 highlanders move to the VL endemic lowlands seasonally every year. Non immune high landers migrate to the low land VL endemic areas searching for job. In contrast, children are predominantly affected in the other endemic areas in the country like Omo Valley among stable residents. There is no mass population movement seen in this region. |
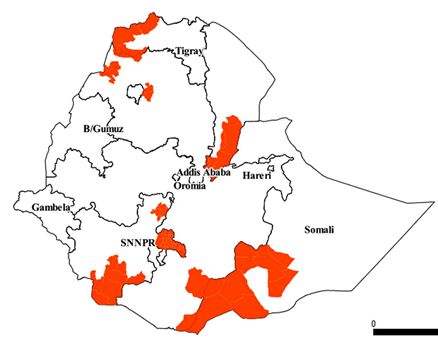 |
| Map 2: The geographic distribution of VL in Ethiopia. (map taken from Leta S, Dao THT, Mesele F, Alemayehu G (2014) Visceral Leishmaniasis in Ethiopia: An Evolving Disease. PLoS Negl Trop Dis 8(9): e3131. doi:10.1371/journal. pntd.0003131.g002) |
References:
Alvar J et al, Leishmaniasis worldwide and Global estimates of its incidence. PlosOne 7 (5) 2012
WHO, weekly epidemiological record. 3 June 2016. No 22, 91 (285-296)
Guidelines for diagnosis, treatment and prevention of leishmaniasis in Ethiopia, 2nd Ed. June 2013
Wondimeneh Y et al. Trend analysis of visceral leishmaniasis at Addis Zemen Health Center, Northwest Ethiopia, Biomedical research international. 2014